
Most pharmacies have some order. But the gap between a pharmacy that looks arranged and one that genuinely functions well comes down to four things: a logical classification system, a compliant and practical layout, the right storage fixtures, and maintenance routines that actually hold.
This guide walks through all five steps to organise a pharmacy effectively, covers what you need before you begin, and flags the mistakes that undo otherwise good setups.
Key Takeaways
- Effective pharmacy organisation follows five steps: audit stock, zone the space, classify medications, fit the right shelving, and assign maintenance ownership.
- Separate Rx from OTC, group by route of administration, then arrange each group alphabetically by INN.
- Apply FEFO (First Expired, First Out) — nearest expiry dates always go to the front of every shelf.
- Cold chain items require 2–8°C storage; controlled substances must go in lockable, access-restricted cabinets.
- Organisation degrades without ownership — assign named staff to every recurring task.
How to Organise a Pharmacy: Step-by-Step
Step 1: Audit and Declutter Your Existing Inventory
Before rearranging anything, you need an accurate picture of what you actually have.
Physically go through all stock and remove:
- Expired medications (dispose of through authorised channels — not waste bins)
- Discontinued product lines
- Items that haven't moved within your defined review period
- Damaged or compromised packaging
WHO TRS 961 Annex 9 recommends physical inventories be conducted and reconciled with stock records at least twice a year for time- and temperature-sensitive pharmaceutical products — a useful benchmark for any structured audit cycle.
Once stock is cleared, assess your physical storage capacity. Look specifically for:
- Shelves that are overcrowded or double-stacked
- Products stored on the floor (even temporarily)
- Items mixed across unrelated categories
- Zones where FEFO discipline has clearly broken down
These areas become your reorganisation priorities. Don't move on to layout planning until this step is complete — reorganising around hidden clutter wastes time and creates new compliance risk.
Step 2: Plan Your Pharmacy Layout in Functional Zones
A well-organised pharmacy divides physical space into clearly defined zones, each with a distinct function:
| Zone | Purpose |
|---|---|
| OTC/Retail Area | Customer-accessible shelving for vitamins, cold/flu, pain relief, personal care |
| Prescription Dispensing Counter | Staff-only area for Rx verification and dispensing |
| Pharmacist Consultation Space | Private area for patient counselling |
| Back-End Storage Room | Bulk inventory, receiving, and quarantine for returned/recalled stock |
| Cold Storage Zone | Refrigeration for vaccines, insulin, and temperature-sensitive products |
Under India's Drugs and Cosmetics Rules (Schedule N), the dispensing department must be at least 6 m² for one pharmacist, with an additional 2 m² per extra pharmacist, and must be physically separated from the public-access area by a barrier. Floors and walls must be smooth, washable, and free of cracks — these are legal requirements, not optional standards.
When mapping patient flow, position high-frequency OTC products (vitamins, analgesics, cold/flu remedies) where customers can locate them without crossing into staff-only dispensing zones. This reduces interruptions during peak hours and keeps workflow clean.
Step 3: Classify and Arrange Medications Logically
Classification logic is the backbone of pharmacy organisation. Get it right and the system runs itself; get it wrong and products drift back to the wrong shelves within days.
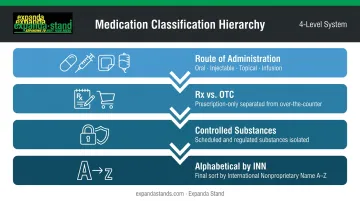
The recommended classification hierarchy:
- Route of administration — separate oral, injectable, topical, infusions, and external-use products into distinct sections
- Rx vs. OTC — never mix prescription and over-the-counter products on the same shelf
- Controlled substances — isolate narcotics and Schedule H/X medications entirely
- Alphabetical by INN — within each sub-group, order by International Nonproprietary Name, not brand name
INN-based labelling matters because brand confusion is a documented source of dispensing errors. A 2025 community pharmacy dispensing error review identified similar drug names as a primary contributor to errors — and a study of 16,539 prescriptions in Latvia found that mandatory INN integration reduced medication error rates from 0.81% to 0.39%.
Apply FEFO rigorously: products with the nearest expiry date go to the front of every shelf, and new stock goes behind. The same review reported that expired medications contributed 21.20% of dispensing errors in one included study — a figure that consistent FEFO discipline directly addresses.
Step 4: Install the Right Storage Fixtures for Each Zone
Fixture selection determines whether your classification system holds in practice. The wrong shelving causes products to drift, slows retrieval, and creates the conditions for picking errors during busy periods.
Match fixture type to zone function:
- OTC/retail area — open gondola shelving or wall-mounted display systems for customer-facing product presentation; adjustable shelf heights accommodate different package sizes
- Prescription dispensing area — enclosed shelving with clear labelling and bin dividers for fast, accurate retrieval
- Controlled substances — lockable cabinets accessible only to the licensed pharmacist in charge; Schedule N requires a clearly labelled poison cupboard with lock and key, with keys held by the responsible person
- Cold chain — pharmaceutical-grade refrigeration rated to maintain 2–8°C consistently for vaccines, insulin, and biologics
- Bulk and back-of-store — raised shelving or pallets to keep products off the floor and protected from humidity
For the OTC retail and dispensing areas, Expanda Stand's pharmacy shelving range — including wall-mounted systems with 8mm toughened glass shelves and 50mm pitch adjustment, gondola units, and enclosed display cabinets with gas spring mechanisms — offers modular configurations that can be customised to fit specific floor plans and product volumes. The modular design also means individual sections can be reconfigured as your product range or floor plan changes, without replacing the entire fixture.
Ensure aisle widths between shelving units allow unobstructed staff movement, particularly during high-traffic periods when retrieval speed is critical.
Step 5: Label Everything and Build Maintenance Routines
A good classification system fails without labelling that staff can read at speed.
Labelling requirements for each shelf position:
- Drug name (INN)
- Category and sub-category
- Dosage form
- Temperature zone (if applicable)
A colour-coded system — one colour per drug category or storage zone — reduces picking errors significantly during busy periods. It also makes it immediately obvious when a product has been returned to the wrong location.
Recurring maintenance schedule:
| Frequency | Task | Owner |
|---|---|---|
| Daily | Shelf tidying, facing, and visual FEFO check | Dispensing staff |
| Weekly | Restocking, near-expiry spot checks, temperature log review | Senior pharmacist |
| Monthly | Full inventory reconciliation, zone audit | Pharmacist in charge |
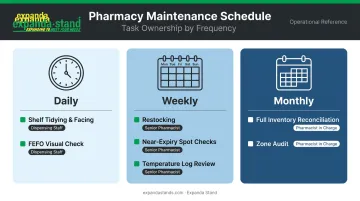
Assign a named person to each task. Shared responsibility produces uneven upkeep — problems surface slower, and accountability is harder to trace.
Before You Begin: What You Need
Attempting to reorganise without preparation creates temporary compliance gaps and wastes the effort entirely. A structured assessment phase comes first.
Equipment and Fixtures Required
Before any physical reorganisation begins, confirm you have:
- Adjustable open shelving — for OTC and retail product display
- Enclosed or lockable cabinets — for Schedule H/X and controlled substances
- Pharmaceutical-grade refrigeration — rated to hold 2–8°C reliably, with temperature monitoring capability
- Labelling tools — label printer or pre-printed shelf tags with INN and category fields
- Bin dividers and drawer inserts — for smaller items, syringes, and accessories
- Pallets or raised shelving bases — to keep all stock off the floor
The scale and type of fixtures should match your floor plan and product range volume. A pharmacy carrying 300 SKUs has different shelving needs than one carrying 1,500.
Regulatory and Compliance Readiness
Review the applicable regulations before moving a single shelf unit. In India, the primary framework is the Drugs and Cosmetics Act and Rules, including Schedule N premises requirements and Rule 65 prescription and register controls for Schedule H/H1/X medications.
Before finalising your layout, confirm the following compliance checkpoints:
- Storage separation: Verify which drug categories require dedicated, physically separate storage zones
- Dispensing zone requirements: Confirm counter and restricted-access area specifications for your licence category
- Register controls: Ensure your layout supports Rule 65 register access and documentation workflows
- Inspection readiness: Cross-reference your floor plan against Schedule N premises requirements before committing to any fixture placement
Getting this right at the planning stage avoids costly layout changes after an inspector flags a non-compliant zone.
Key Factors That Determine How Well Your Pharmacy Stays Organised
The initial setup is only as durable as the systems supporting it. Four variables consistently determine whether pharmacy organisation holds over time.
Physical Space and Shelving Configuration
Insufficient or poorly chosen shelving leads directly to floor storage, overcrowding, and FEFO breakdown. The right configuration — adjustable shelf heights, clearly separated OTC and Rx zones, accessible aisles — reduces retrieval time and pick errors during high-traffic hours.
Shelving that cannot accommodate your product range forces staff into workarounds. Those workarounds don't stay temporary — they quietly replace the intended system over time.
Drug Classification System
Without a consistent, staff-understood classification logic, products get returned to the wrong location after every dispensing cycle. Organising by brand name is the most common mistake — brand names change, generics multiply, and staff trained on one brand can't locate a substituted equivalent.
INN-based classification, organised by route of administration, means any trained staff member can locate any product within seconds. That matters most during emergency dispensing or when covering for absent colleagues.
Storage Conditions: Temperature, Humidity, and Light
WHO TRS 961 Annex 9 defines controlled room temperature at approximately 15–25°C and cold chain storage at 2–8°C. Temperature sensors should be accurate to ±0.5°C; temperature records should be checked manually at least twice daily, including weekends.
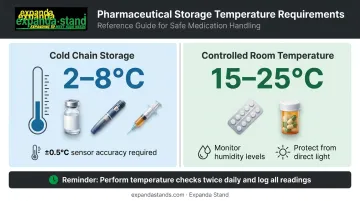
Improper storage degrades drug efficacy before the expiry date is even reached. Vaccines stored outside the cold chain, tablets exposed to humidity, or photosensitive drugs near windows represent patient safety risks — not just stock losses.
Thermometers, hygrometers, and shaded or UV-filtered windows are operational requirements, not optional upgrades.
Staff Training and Role Accountability
FIP/WHO Good Pharmacy Practice guidelines identify medicine supply, advice, and monitoring as core pharmacy activities — all of which depend on staff understanding why the organisational rules exist, not just what they are.
Research on dispensing errors in community pharmacies points to the same causes repeatedly:
- High workload and distractions at peak hours
- Confusion between similar drug names or packaging
- Inadequate processes for stock rotation and retrieval
Training staff on classification logic, FEFO discipline, and cold chain protocols directly addresses all three.
Assign explicit ownership of each task. Named accountability surfaces problems faster than collective responsibility.
Common Mistakes When Organising a Pharmacy
Even well-intentioned pharmacies fall into organisational habits that create compliance gaps and dispensing risks. These are the most common — and most preventable.
- Rx and OTC products stored on the same shelf breach Drugs and Cosmetics Rules (Rule 65) controls for Schedule H/H1/X medications and sharply raise dispensing error risk during busy periods.
- Floor storage sold to staff as "temporary" rarely stays that way. Schedule N mandates clean, washable storage surfaces — and within weeks, floor stacks become a permanent humidity and compliance hazard.
- Skipping FEFO because rotating stock is inconvenient is the leading cause of expired medications reaching patients. One habit fixes it: new stock always goes behind existing stock, no exceptions.
- No documented maintenance schedule means upkeep happens inconsistently, problem areas get missed, and the facility deteriorates between inspection cycles. Assign names, set dates, and review the schedule monthly.
Conclusion
Organising a pharmacy effectively is not a one-time project. It requires a logical classification system, compliant and well-fitted storage infrastructure, and consistent maintenance routines — and all three need to work together.
Most organisational failures trace back to skipping the planning phase, using fixtures that don't match the product range, or assigning no clear ownership to upkeep. The five steps in this guide address each of those failure points directly.
A well-organised pharmacy dispenses faster, makes fewer errors, and passes compliance checks without scrambling. Getting there comes down to the right shelving layout, the right storage infrastructure, and clear staff accountability — three things worth investing in before problems force the issue.
Frequently Asked Questions
What are the 5 pillars of pharmacy?
FIP/WHO's Good Pharmacy Practice framework defines five pillars: patient welfare, supply of quality medicines, advice and monitoring, rational medicine use, and professional accountability. A well-organised pharmacy actively supports each pillar by reducing dispensing errors, maintaining correct storage conditions, and keeping the working environment compliant.
How should medications be arranged on pharmacy shelves?
Medications should be arranged by route of administration (oral, injectable, topical), separated into Rx and OTC categories, and ordered alphabetically by International Nonproprietary Name within each group. Apply the FEFO principle so products with the nearest expiry dates are always positioned at the front of each shelf.
What is the FEFO principle and why does it matter in pharmacy?
FEFO (First Expired, First Out) requires medicines with the earliest expiry date to be placed at the front of the shelf and dispensed first. It prevents newer stock from sitting in front while older batches expire behind it — a documented cause of expired medication reaching patients.
How do you store controlled substances in a pharmacy?
Narcotics and Schedule H/X drugs must be kept in dedicated, lockable cabinets accessible only to the licensed pharmacist in charge. Schedule N substances require a clearly labelled poison cupboard; WHO guidance specifies that all narcotics and psychotropics be held in securely locked facilities with every movement recorded.
What storage conditions must a pharmacy maintain for temperature-sensitive medicines?
Vaccines, insulin, and biologics require cold chain storage between 2–8°C in a pharmaceutical-grade refrigerator. Standard medicines should be stored at controlled room temperature (approximately 15–25°C), away from direct sunlight, heat sources, and humidity. Temperature records should be checked at least twice daily.
How often should a pharmacy reorganise its shelving and storage?
At minimum: tidy shelves daily, restock and run near-expiry spot checks weekly, and complete a full inventory reconciliation monthly. Revisit your overall layout whenever product range, stock volume, or physical space changes significantly.


